
Treating diabetic retinopathy
There are a number of treatment options for diabetic retinopathy (DR). These treatment options will depend on the type and extent of your condition.
Your ophthalmologist will consult with you to determine the best treatment for your particular circumstances. However, here are the most common courses of treatment for diabetic retinopathy.
Fenofibrate
The drug Fenofibrate has been shown to reduce the risk of DR progression by about 30 per cent for some people with existing non-proliferative diabetic retinopathy (NPDR).
Fenofibrate is often used to treat high blood lipid levels. However, it appears to provide benefit even for people who have normal lipid levels.1
If you’re not already taking this drug, and have diabetic retinopathy, ask your general practitioner, endocrinologist or ophthalmologist whether this treatment may be suitable for you.
Treating diabetic retinopathy with laser
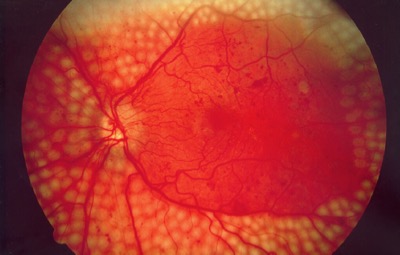
For most people with proliferative diabetic retinopathy, laser treatment is the most effective treatment. Laser treatment is also known as panretinal photocoagulation (PRP). PRP treatment has been shown to halve the risk of severe vision loss in people with PDR.
Typically, between 1,000 and 2,000 laser spots are applied to the retina, away from the macula, over several appointments. This reduces oxygen demand of the peripheral parts of the retina.
PRP laser treatment can also reduce the production of a protein called vascular endothelial growth factor (VEGF). VEGF is predominantly responsible for the abnormal growth of blood vessels and fluid leakage under the retina.
Laser treatment is typically performed in an outpatient clinic by an ophthalmologist. Most people tolerate laser treatment very well, but some may experience discomfort.
Drops are needed to dilate the pupils for laser treatment. This can cause some blurring of vision for several hours, so you’ll need someone to take you home, because you won’t be able to drive.
Intravitreal injections
An intravitreal injection (sometimes referred to as IVI or an eye injection) involves the injection of a medication into the eye. This is usually an anti-inflammatory steroid, or a medication that blocks VEGF (these are often referred to as anti-VEGF).
IVI is often used to treat diabetic macular oedema. In many cases, these injections can stabilise or improve vision. Intravitreal anti-VEGFs may sometimes be used to treat PDR.
It’s important to know that injections usually need to be repeated often, up to each month, for many months, to ensure the best outcomes.
The choice of medication and treatment interval will be determined by your ophthalmologist.
Watch: What to expect at an eye injection

Eye injection quick facts
Regardless of which medication is used, the following points apply:
- An anaesthetic eye drop and cleaning solution are applied to the eye before the injection.
- You should experience very little pain, if any, during the procedure.
- It’s a quick procedure and usually occurs in your ophthalmologist’s rooms, although some patients may be treated in a day-stay unit.
- Treatment usually begins with injections at monthly intervals, but may be given less frequently once the swelling is controlled.
- Even if your vision stabilises or improves you may still need to continue treatment.
- Treatment depends on each person’s individual medical circumstances. So, you’re encouraged to discuss your treatment plan with your ophthalmologist.
- You should always follow your treatment schedule and only stop treatment when advised by your eye health professional.
- Any sudden changes in vision or difficulties experienced after your injection, such as increasing eye redness or persistent pain, should be reported to your ophthalmologist immediately. Although rare, infection within the eye can occur and this is an emergency.
- Urgent review by an ophthalmologist can save your sight, if an infection occurs.
- You should arrange for someone to take you home after your appointment, because you won’t be able to drive after the procedure.
If you have any concerns or you are having difficulties coping with the treatment, discuss these concerns with your ophthalmologist.
Download

Download this publication today.
DownloadVitrectomy
A vitrectomy involves the surgical removal of the vitreous (central gel cavity) of the eye.
If you’re not seeing an ophthalmologist already, you will be referred to one for the vitrectomy. You will have the procedure in an operating theatre, under either local or general anaesthesia.
Your ophthalmologist may recommend a vitrectomy where there is bleeding into the vitreous (also known as a vitreous haemorrhage). The procedure is also recommended for progressive proliferative diabetic retinopathy (PDR) despite laser and injection treatment. It’s also a treatment for tractional retinal detachments complicating PDR.
Surgery aims to remove the blood and scar tissue from the surface of the retina. Laser is often applied during the treatment as well.
Often, at the end of the procedure, the vitreous is replaced with fluid or a temporary bubble of gas. This gas bubble may take days or weeks to be absorbed. For that reason, your vision may take some time to clear after a vitrectomy.



If you have general questions about treatment for your eye condition, our National Helpline is a good place to start. Our friendly, trained staff can help with information and advice. It’s free.
Contact us
